

Breast Cancer Overview
About Breast Cancer
The female breast is composed of skin, fibrous tissue, breast glands and fat. Breast cancer is a malignant tumor that occurs in the glandular epithelium of the breast. The breast is not an important organ to maintain the life activities of the human body, and breast cancer in situ is not fatal; but because breast cancer cells lose the characteristics of normal cells, the connection between cells is loose and easy to fall off. Once cancer cells fall off, free cancer cells can spread throughout the body with blood or lymph, forming metastasis and life-threatening.
Breast cancer is more common in developed countries, but the survival rate is higher than in developing countries. Globally, breast cancer is the main type of cancer in women, accounting for 25% of all cases, and the incidence of women is more than 100 times higher than that of men. Researchers have determined that hormones, lifestyle and environmental factors may increase the risk of breast cancer. Breast cancer is likely to be caused by a complex interaction between your genetic makeup and the environment.
The global incidence of breast cancer has been on the rise since the late 1970s. One in eight women in the United States will develop breast cancer in their lifetime. Breast cancer has become a major public health problem in the current society. The global mortality rate of breast cancer has shown a downward trend since the 1990s; first, the development of breast cancer screening has increased the proportion of early cases; second, the development of comprehensive treatment of breast cancer has improved the curative effect. These make breast cancer be one of the solid tumors that can be effectively treated.
Overview of breast cancer pathways
Main Signaling Pathways in Breast Cancer
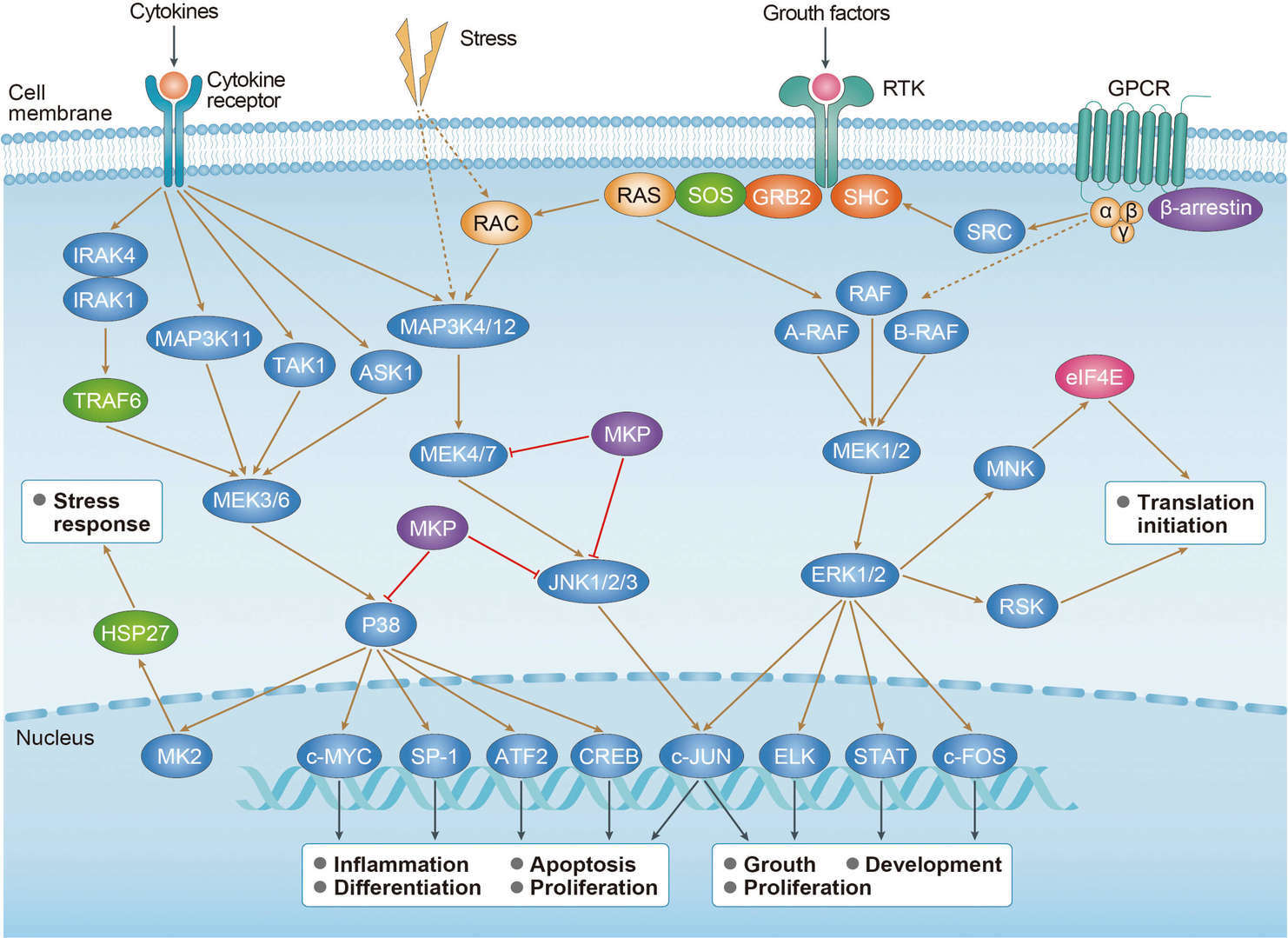 MAPK Pathway
MAPK Pathway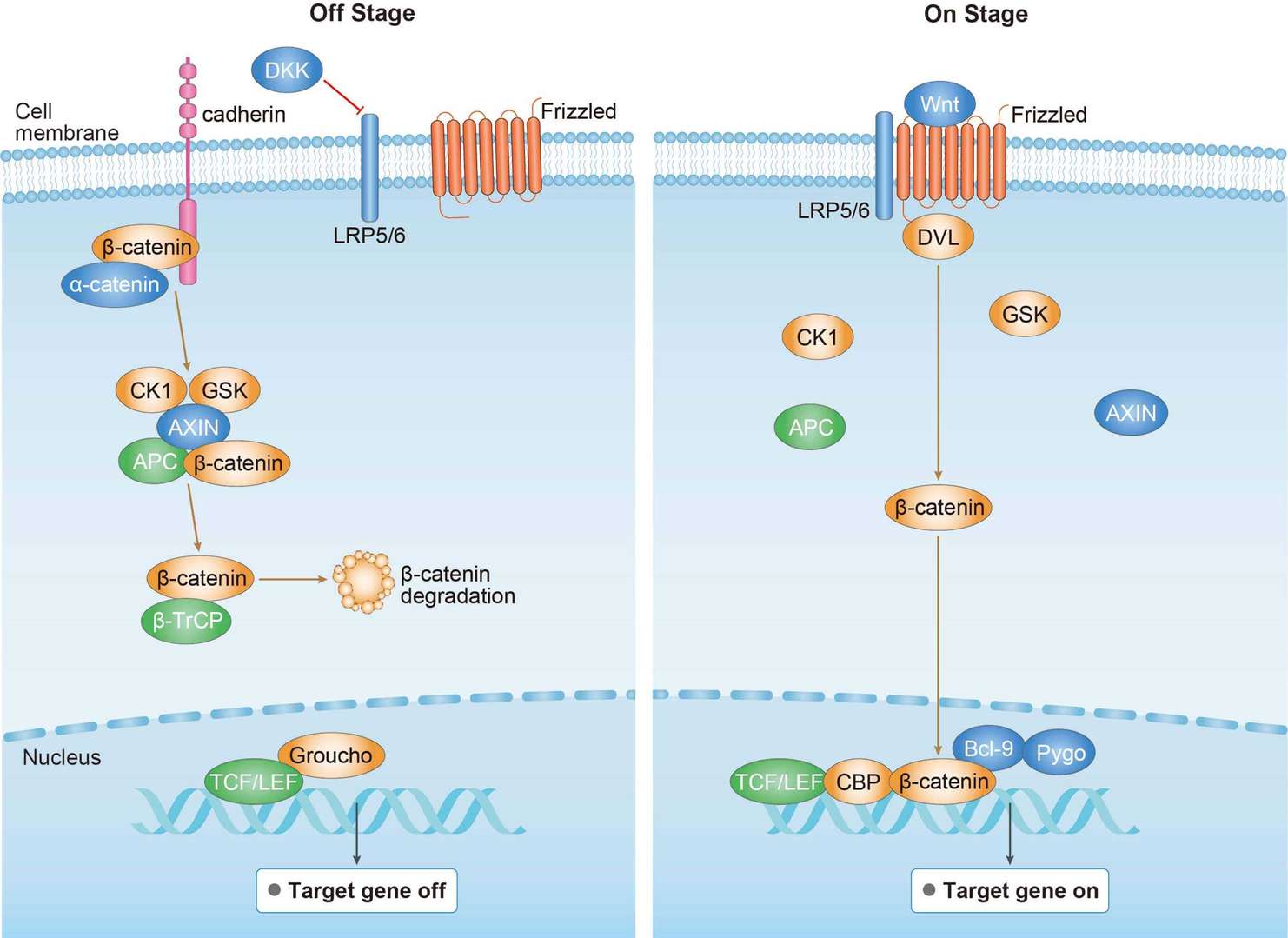 Wnt Pathway
Wnt Pathway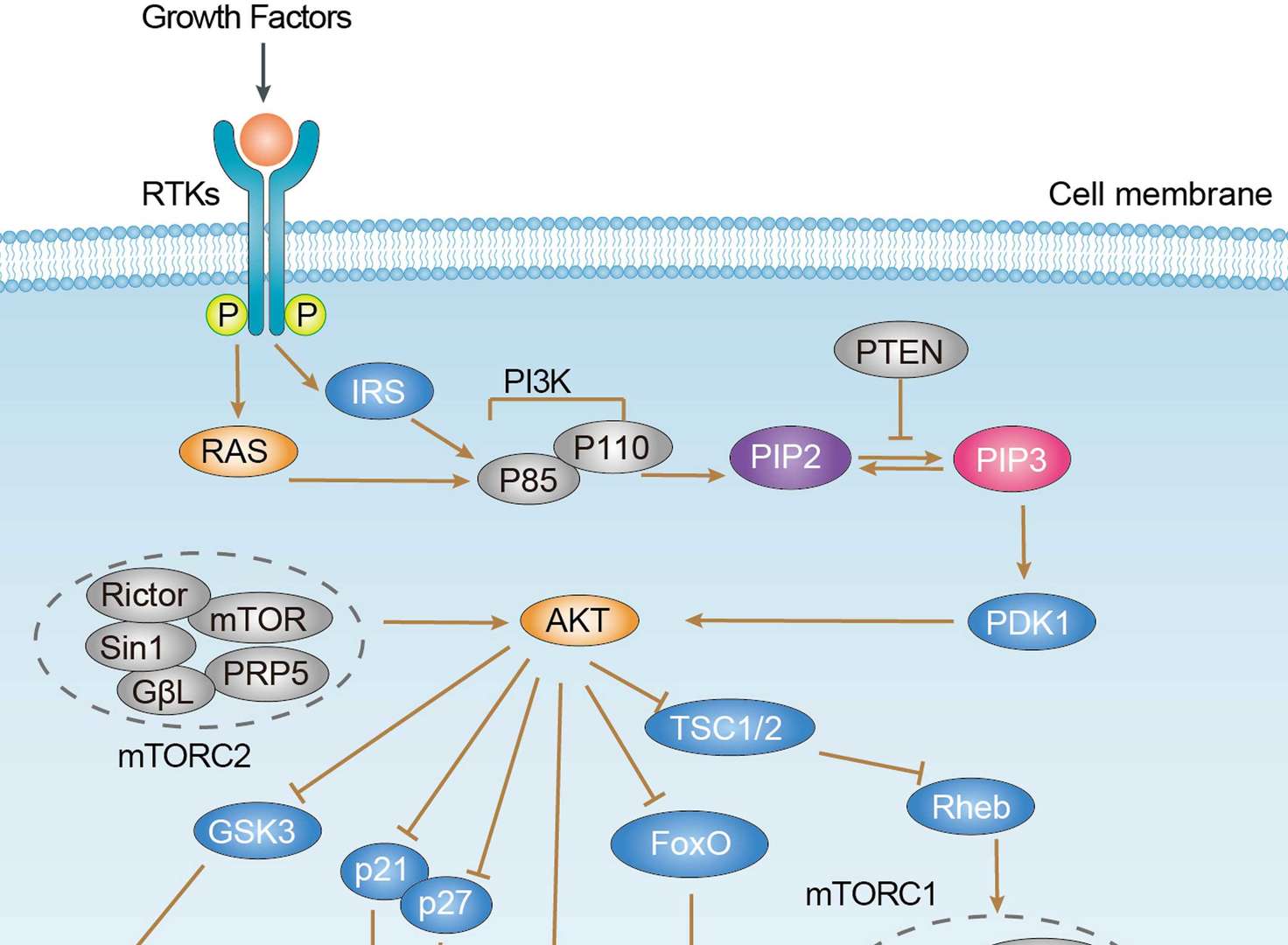 PI3K-Akt Pathway
PI3K-Akt Pathway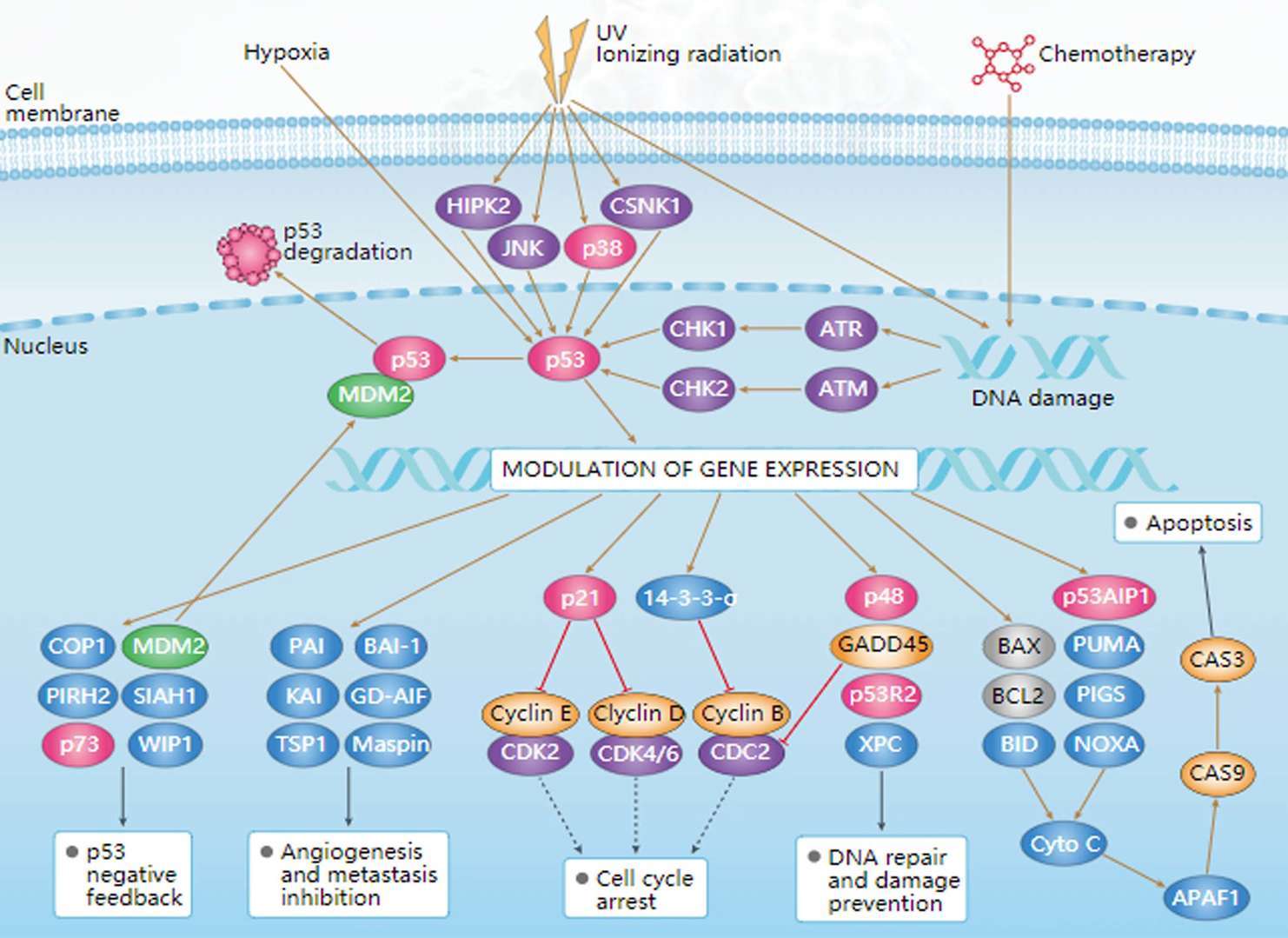 p53 Pathway
p53 Pathway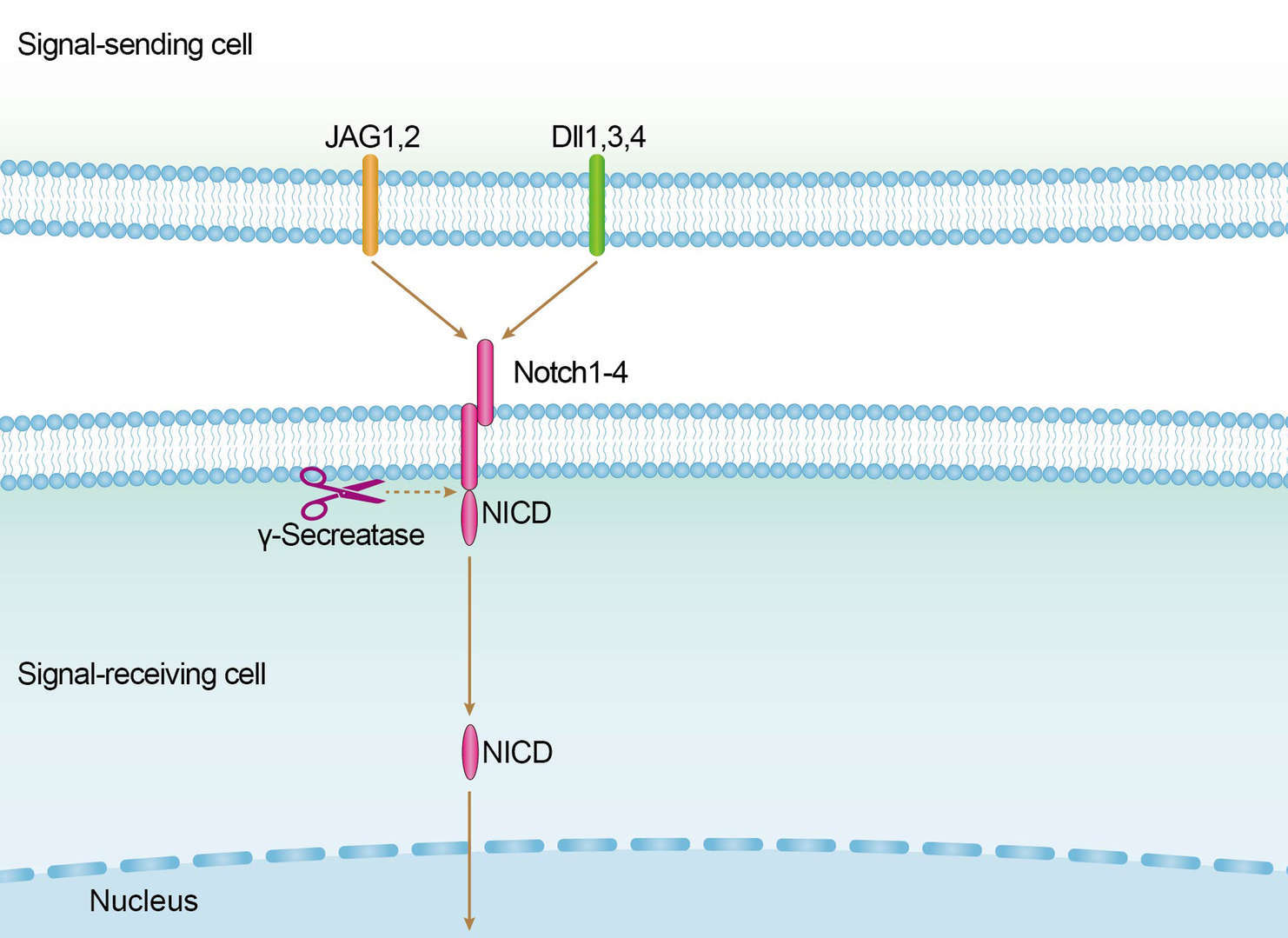 Notch Pathway
Notch PathwayDiagnosis of Breast Cancer
Most types of breast cancer can be easily diagnosed from microscopic samples of breast lesions or biopsies. There remain some types of breast cancer require special laboratory tests. The two most commonly used screening/diagnosis methods, mammography and physical examination, can provide a rough chance that the lump is cancer, and other lesions, such as simple cysts, can be detected. When these tests are inconclusive, healthcare workers can take fluid samples from the mass for microscopic analysis, or fine needle aspiration and cytology (FNAC) to help establish a diagnosis. Needle aspiration can be performed at the health care provider's office or clinic. A local anesthetic can be used during surgery to numb breast tissue to prevent pain, but if the lump is not under the skin, it may not be necessary. It is found that clear fluid makes the mass highly unlikely to be cancerous, but bloody fluid may be sent to examine cancer cells under a microscope. Together, physical examination of the breast, mammography and FNAC can be used to diagnose breast cancer with high accuracy.
Other biopsy options include a core biopsy or vacuum-assisted breast biopsy, which is the procedure in which part of the breast mass is removed, or an excision biopsy to remove the entire mass. In general, the results of physical examinations by health care providers, mammograms and other examinations that may be performed in special circumstances are sufficient to ensure that resection biopsies are performed as definitive diagnosis and primary treatment.
Targeted Therapy for Breast Cancer
Targeted therapy for breast cancer uses drugs that prevent the growth of breast cancer cells in specific ways. In about 1/5 of women with breast cancer, there is too much growth-promoting protein, called human epidermal growth factor receptor 2 (HER2), on the surface of the cancer cells. These cancers, known as HER2-positive breast cancers, tend to grow and spread more aggressively. Many drugs have been developed to target this protein. Trastuzumab (Herceptin) is a monoclonal antibody usually used alone or in conjunction with chemotherapy for the treatment of early and advanced breast cancer. It usually takes six months to a year to start using the drug before (neoadjuvant) surgery (neoadjuvant) or after (adjuvant) surgery for early breast cancer. For advanced breast cancer, it is usually treated as long as the drug helps. Pertuzumab (Perjeta) is another monoclonal antibody that can be used in combination with trastuzumab and chemotherapy before or after surgery to treat early or advanced breast cancer. Ado-trastuzumab Emtansine (Kadcyla or TDM-1) is an antibody-drug conjugate consisting of the trastuzumab (Herceptin) covalently linked to the cytotoxic agent DM1. It has been used alone to treat early or advanced breast cancer in women who have received trastuzumab and chemotherapy. Lapatinib (Tykerb) is used in the treatment of advanced breast cancer and may be used in combination with certain chemotherapy drugs or hormone therapies. Nelatinib (Nerlynx) is another kinase inhibitor. This is the medicine I take every day. Nelatinib is used to treat breast cancer in a woman who has completed trastuzumab treatment for one year.
Palbociclib (Ibrance), ribociclib (Kisqali) and abemaciclib (Verzenio) are drugs that can block intracellular proteins, called cyclin-dependent kinase (CDK), especially CDK4 and CDK6. Blocking these proteins in hormone receptor-positive breast cancer cells can help prevent cell division slow the growth of cancer. Everolimus is used in postmenopausal women with hormone receptor-positive, HER2-negative breast cancer. It is used in conjunction with Aremassin, an aromatase inhibitor, for women whose cancers have increased while being treated with letrozole or anastrozole. In addition, other targeted drugs include Olaparib (Lynparza) and talazoparib (Talzenna) known as poly ADP-ribose polymerase (PARP) inhibitors, and Alpelisib (Piqray) known as a phosphoinositide 3-kinase (PI3K) inhibitor.
For research use only. Not intended for any clinical use.
Send Inquiry
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.