
Thyroid Cancer Overview - Signaling Pathway. Diagnosis. Targeted Therapy
About Thyroid Cancer
Thyroid cancer is cancer that develops from the tissues of the thyroid gland. It is a disease in which cells grow abnormally and have the potential to spread to other parts of the body. Symptoms can include swelling or a lump in the neck. Cancer can also occur in the thyroid after spread from other locations, in which case it is not classified as thyroid cancer. Risk factors include radiation exposure at a young age, having an enlarged thyroid, and family history. The four main types are papillary thyroid cancer, follicular thyroid cancer, medullary thyroid cancer, and anaplastic thyroid cancer. Diagnosis is often based on ultrasound and fine needle aspiration. Screening people without symptoms and at normal risk for the disease is not recommended as of 2017.Thyroid cancers are thought to be related to a number of environmental and genetic predisposing factors, but significant uncertainty remains regarding their causes. Environmental exposure to ionizing radiation from both natural background sources and artificial sources is suspected to play a significant role, and significantly increased rates of thyroid cancer occur in those exposed to mantle field radiation for lymphoma, and those exposed to iodine-131 following the Chernobyl, Fukushima, Kyshtym, and Windscale nuclear disasters. Thyroiditis and other thyroid diseases also predispose to thyroid cancer. Genetic causes include multiple endocrine neoplasia type 2, which markedly increases rates, particularly of the rarer medullary form of the disease. The American Cancer Society’s most recent estimates for thyroid cancer in the United States for 2018 are: about 53,990 new cases of thyroid cancer (40,900 in women, and 13,090 in men) and about 2,060 deaths from thyroid cancer (1,100 women and 960 men).
Overview of thyroid cancer pathways
Main Signaling Pathways in Thyroid Cancer
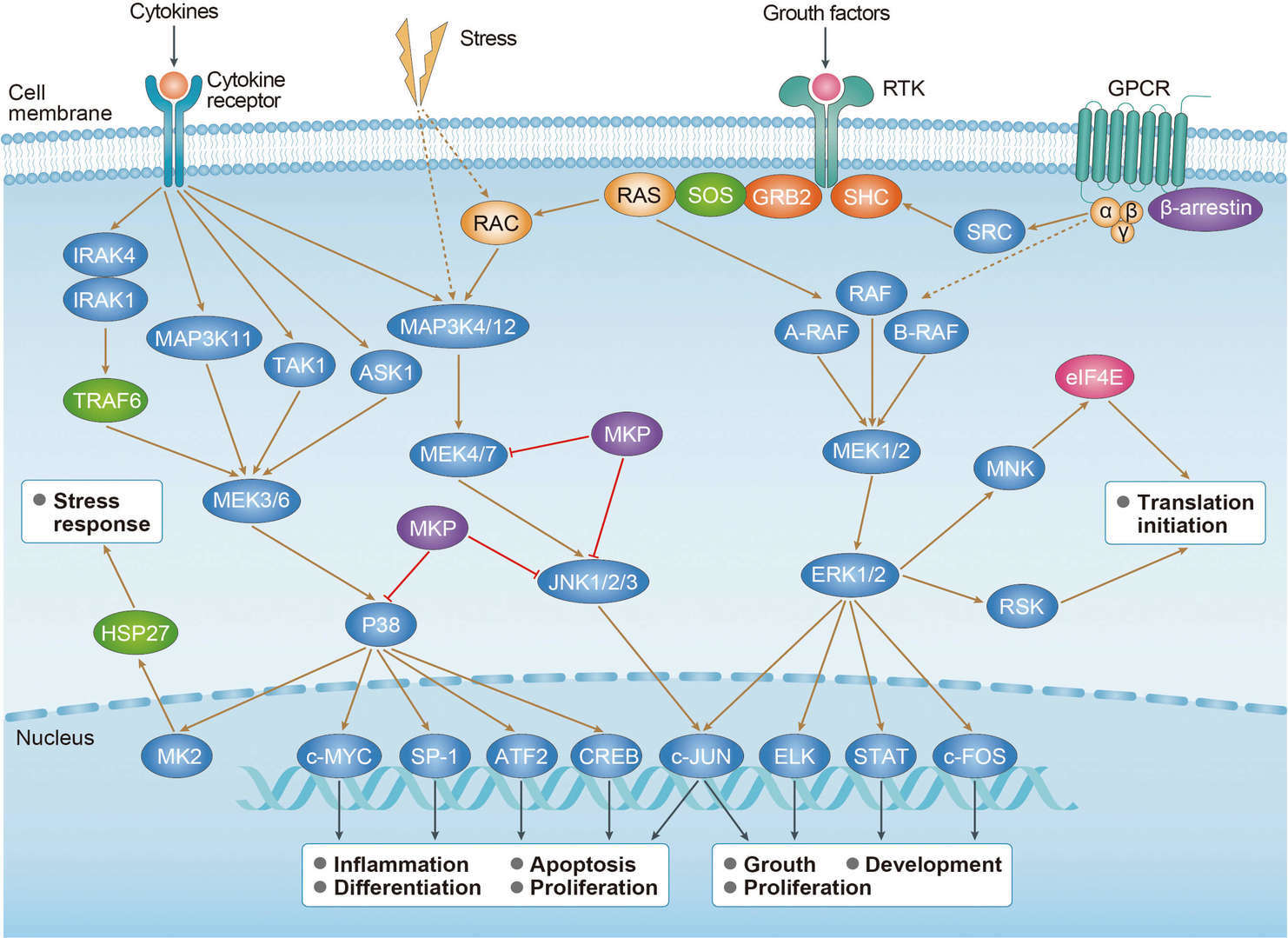 MAPK Pathway
MAPK Pathway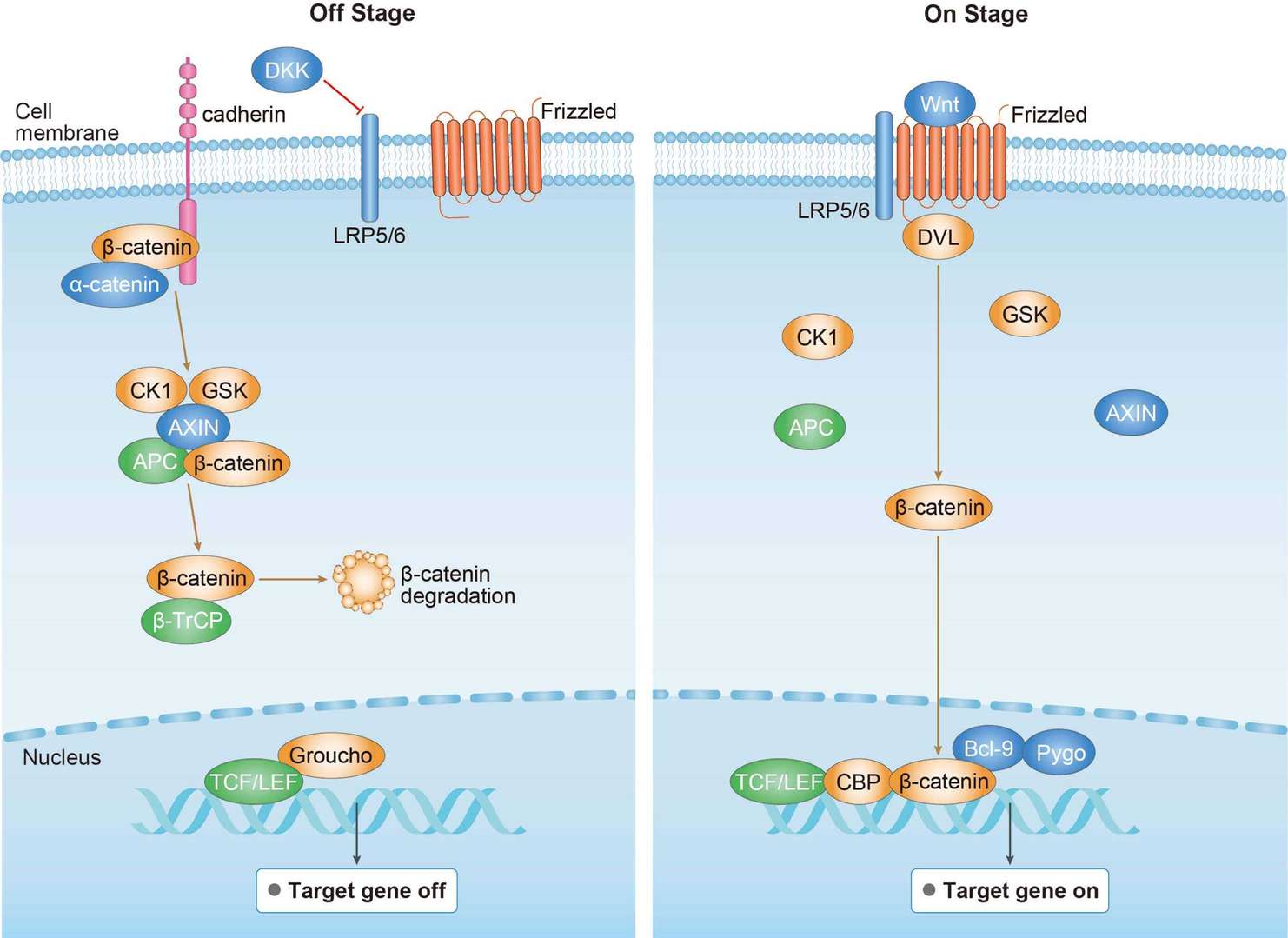 Wnt Pathway
Wnt Pathway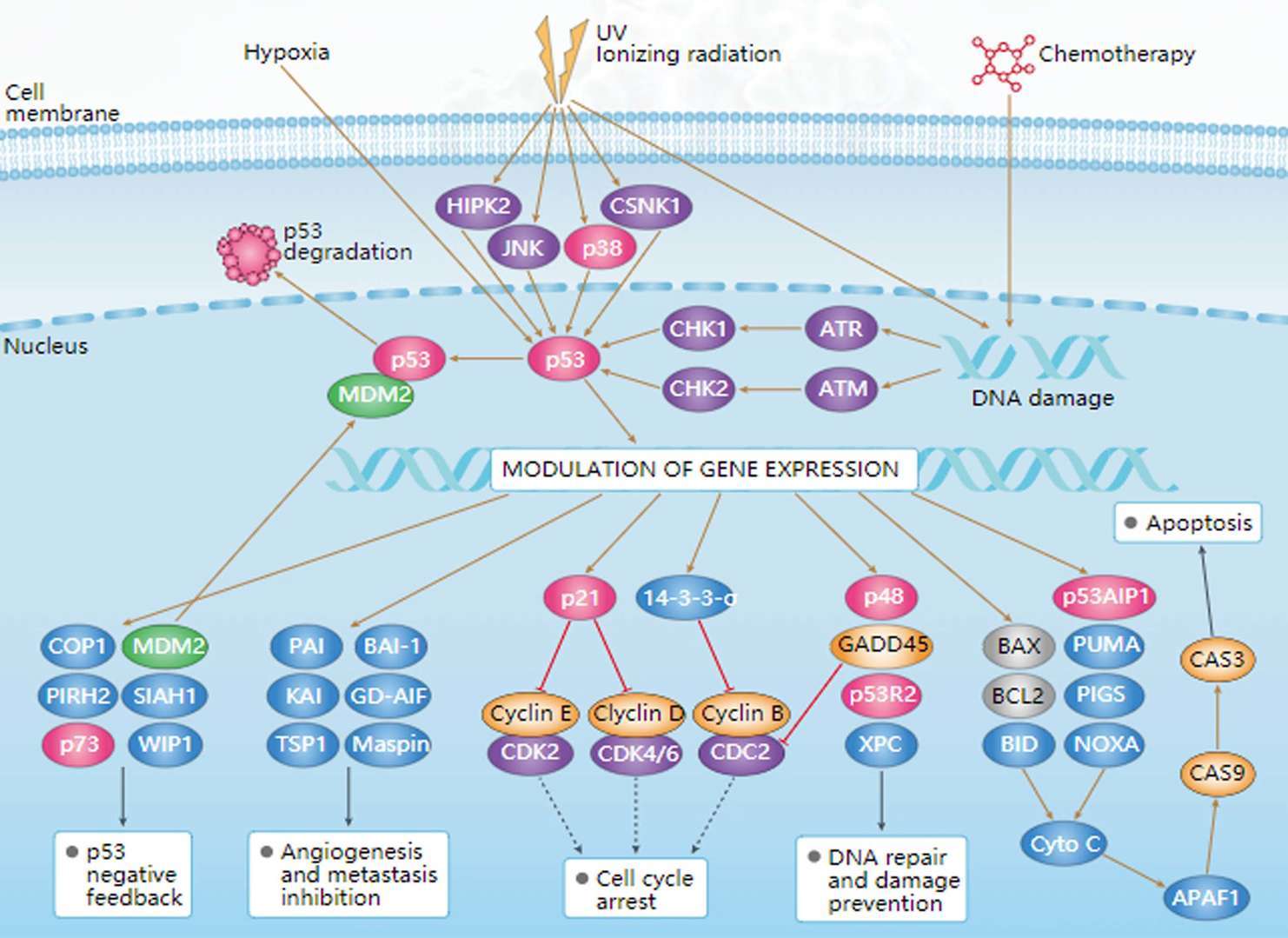 p53 Pathway
p53 Pathway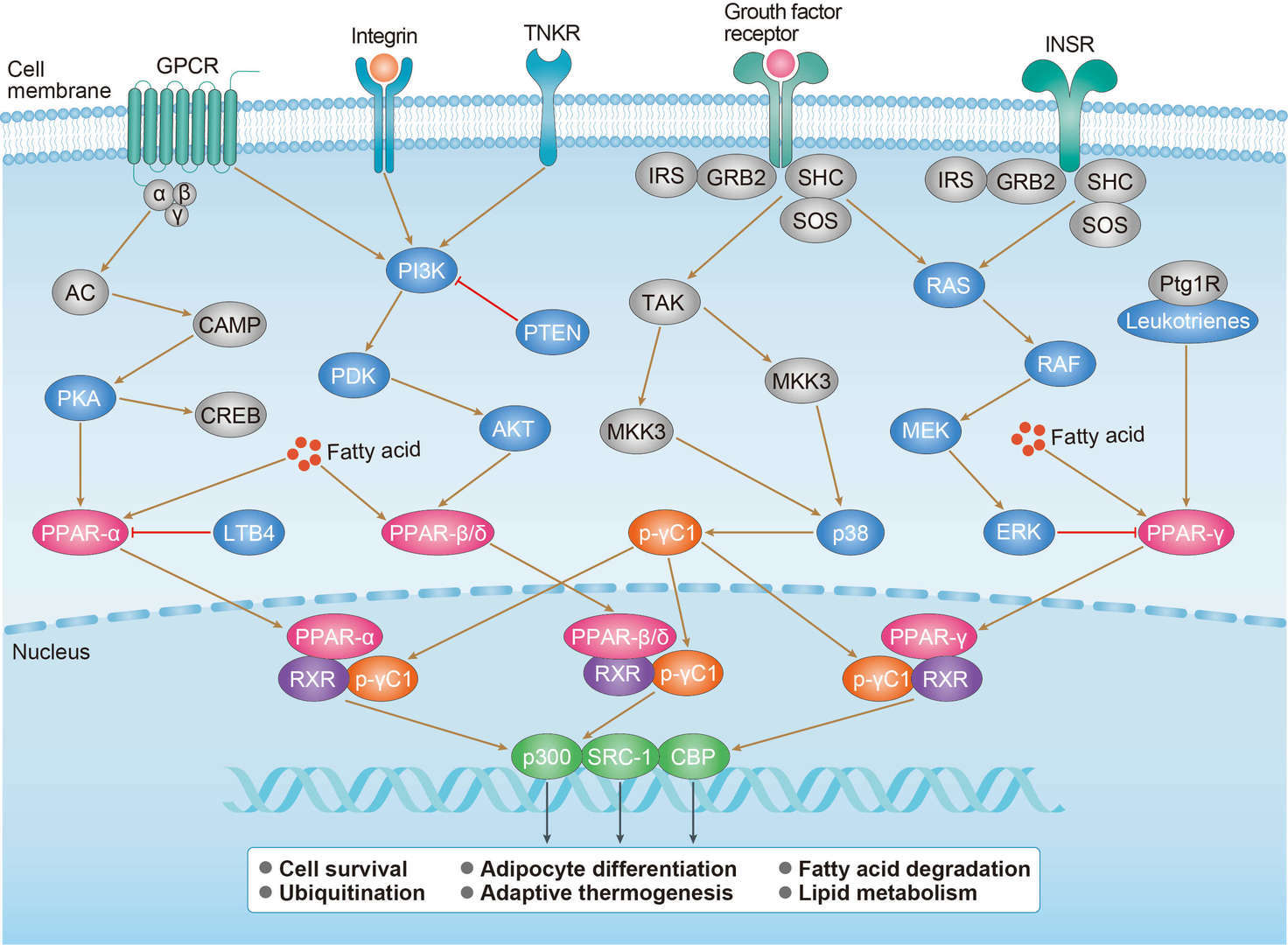 PPAR Pathway
PPAR PathwayDiagnosis of Thyroid Cancer
Thyroid nodules are of particular concern when they are found in those under the age of 20. The presentation of benign nodules at this age is less likely, thus the potential for malignancy is far greater. After a thyroid nodule is found during a physical examination, a referral to an endocrinologist or a thyroidologist may occur. Most commonly, an ultrasound is performed to confirm the presence of a nodule and assess the status of the whole gland. Measurement of thyroid stimulating hormone and anti-thyroid antibodies will help decide if a functional thyroid disease such as Hashimoto's thyroiditis is present, a known cause of a benign nodular goiter. Measurement of calcitonin is necessary to exclude the presence of medullary thyroid cancer. Finally, to achieve a definitive diagnosis before deciding on treatment, a fine needle aspiration cytology test is usually performed and reported according to the Bethesda system. In adults without symptoms, screening for thyroid cancer is not recommended.
Targeted Therapy for Thyroid Cancer
Vandetanib (Caprelsa) is a targeted drug taken as a pill once a day. In patients with advanced MTC, vandetanib stops cancers from growing for an average of about 6 months, although it is not yet clear if it can help people live longer. Cabozantinib (Cometriq) is another targeted drug used to treat MTC. It is taken in pill form once a day. In MTC patients, cabozantinib has been shown to help stop cancers from growing for about 7 months longer than a sugar pill. So far, though, it has not been shown to help patients live longer. Sorafenib (Nexavar) and lenvatinib (Lenvima) are targeted drugs known as kinase inhibitors. They work in 2 ways. They help block tumors from forming new blood vessels, which the tumors need to grow. These drugs also target some of the proteins made by cancer cells that normally help them grow. Dabrafenib (Tafinlar) and trametinib (Mekinist) are drugs that target some of these proteins. These drugs can be used together to treat anaplastic thyroid cancers that have a certain type of BRAF gene change and that can’t be removed completely with surgery.
References
1. Benvenga, S.; Koch, CA. Molecular pathways associated with aggressiveness of papillary thyroid cancer. Current Genomics. 2014 Jun; 15(3): 162-70.
2. Ferrari, SM.; et al. Molecular Targeted Therapies of Aggressive Thyroid Cancer. Frontiers in Endocrinology. 2015 Nov 20; 6: 176.
3. Naoum, GE.; et al. Novel targeted therapies and immunotherapy for advanced thyroid cancers. Molecular Cancer. 2018 Feb 19; 17(1): 51.
4. Jin, S.; et al. Signaling Pathways in Thyroid Cancer and Their Therapeutic Implications. Journal of Clinical Medicine Research. 2016 Apr; 8(4): 284-96.
5. Davies, TF.; Latif, R. Targeting the thyroid-stimulating hormone receptor with small molecule ligands and antibodies. Expert Opinion on Therapeutic Targets. 2015 Dec 21; 5: 288.
6. Liu, M.; et al. Update on the molecular diagnosis and targeted therapy of thyroid cancer. Medical Oncology. 2014 Jun; 31(6): 973.
7. KEGG PATHWAY: Thyroid cancer - Homo sapiens (human).
For research use only. Not intended for any clinical use.
Send Inquiry
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.