

Motavizumab Overview
Introduction of Motavizumab
Motavizumab (MEDI-524) is a humanized IgG1 monoclonal antibody (mAb). It is being investigated for the prevention of respiratory syncytial virus (RSV) infection in high-risk infants.
Mechanism of Action of Motavizumab
Motavizumab differs from palivizumab, its marketed predecessor, by 13 amino acid residues. Both mAbs target a highly conserved antigenic site A on the fusion (F) glycoprotein of RSV, but motavizumab has greater neutralizing activity compared to palivizumab. RSV F is a class I fusion glycoprotein that is synthesized as an inactive precursor (F0) that is processed by a furin-like protease at two sites to generate three polypeptides: the N-terminal fragment (F2), a 27-amino-acid glycopeptide (pep27) and the C-terminal fragment (F1). The mature, active protein exists as a trimer of F2-F1 heterodimers folded into a compact prefusion conformation. The process of membrane fusion begins once prefusion RSV F is triggered by an unknown mechanism to initiate a dramatic conformational change. This refolding can also occur spontaneously on virions and cell surfaces, and it can be stimulated with heat, indicating that prefusion RSV F is metastable. During the refolding, the hydrophobic fusion peptide at the N terminus of the F1 subunit pulls out from the central cavity of the prefusion trimer and inserts into the host-cell membrane. The resulting pre-hairpin intermediate then further refolds as the heptad repeats adjacent to the fusion peptide (HRA) associate with the heptad repeats adjacent to the viral transmembrane region (HRB), located near the C terminus of the F1 subunit. This association leads to the formation of an extremely stable six-helix bundle, which is characteristic of the RSV F postfusion conformation and brings the viral and host-cell membranes together. Inhibition of any of these steps during the fusion process may prevent entry and infection of the host cells and could thus serve as a target for therapeutic intervention. Motavizumab acts by binding the RSV F protein on the surface of the virus and blocking a critical step in the membrane fusion process.
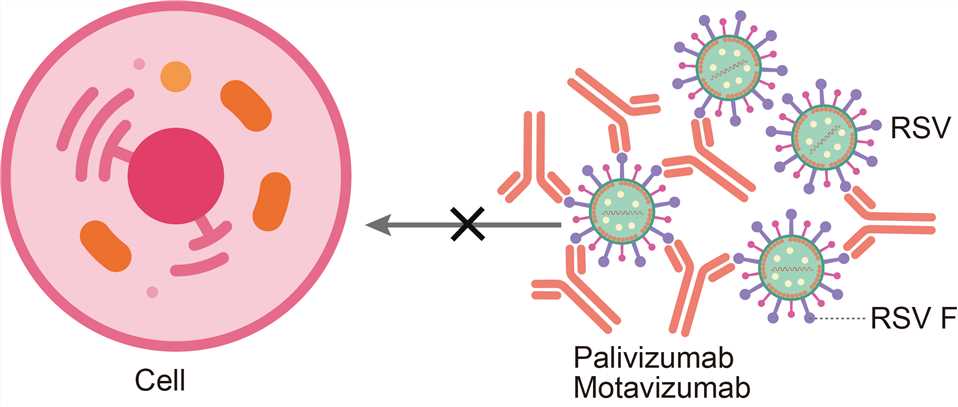
Fig.1 Mechanism of action of Motavizumab
For research use only. Not intended for any clinical use.
Send Inquiry
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.