

Graft-versus-host Disease Overview
Graft-versus-host disease (GvHD) is an immune condition that occurs in patients after transplantation. It is specifically manifested by immune cells present in the donor tissue (graft) attacking the host's own tissue. The disease is allogeneic bone marrow common side effects after transplantation (stem cell transplantation). Allogeneic transplantation refers to the transplantation of bone marrow tissue or cells from a donor. It is a common treatment for many different cancers, including cancers that affect blood and lymph nodes, and other non-cancer diseases that affect blood or immune system. In addition to bone marrow transplant surgery, GvHD can also occur after a solid organ transplant that may contain cells of the immune system, such as white blood cells.
Introduction of GvHD
There are two types of GvHD: acute graft-versus-host disease (aGvHD) and chronic graft-versus-host disease (cGvHD), whose symptoms range from mild to severe and life-threatening, and usually include skin inflammation, jaundice and gastrointestinal upset, and other organ problems. Acute GVHD usually occurs within the first 100 days after transplantation. It causes clinical symptoms of rash, liver disease, and intestinal symptoms such as nausea and diarrhea. Chronic GVHD occurs later; it generally affects many different organs and body systems. GvHD has a complex pathophysiology that involves many interactions between transplanted donor and recipient patient immune cells. Although some measures can be taken to reduce the risk after the occurrence of GvHD, effective prevention methods still required to further explore.
Overview of autoimmune thyroid disease pathways
Main Signaling Pathways in GvHD-versus-host Disease
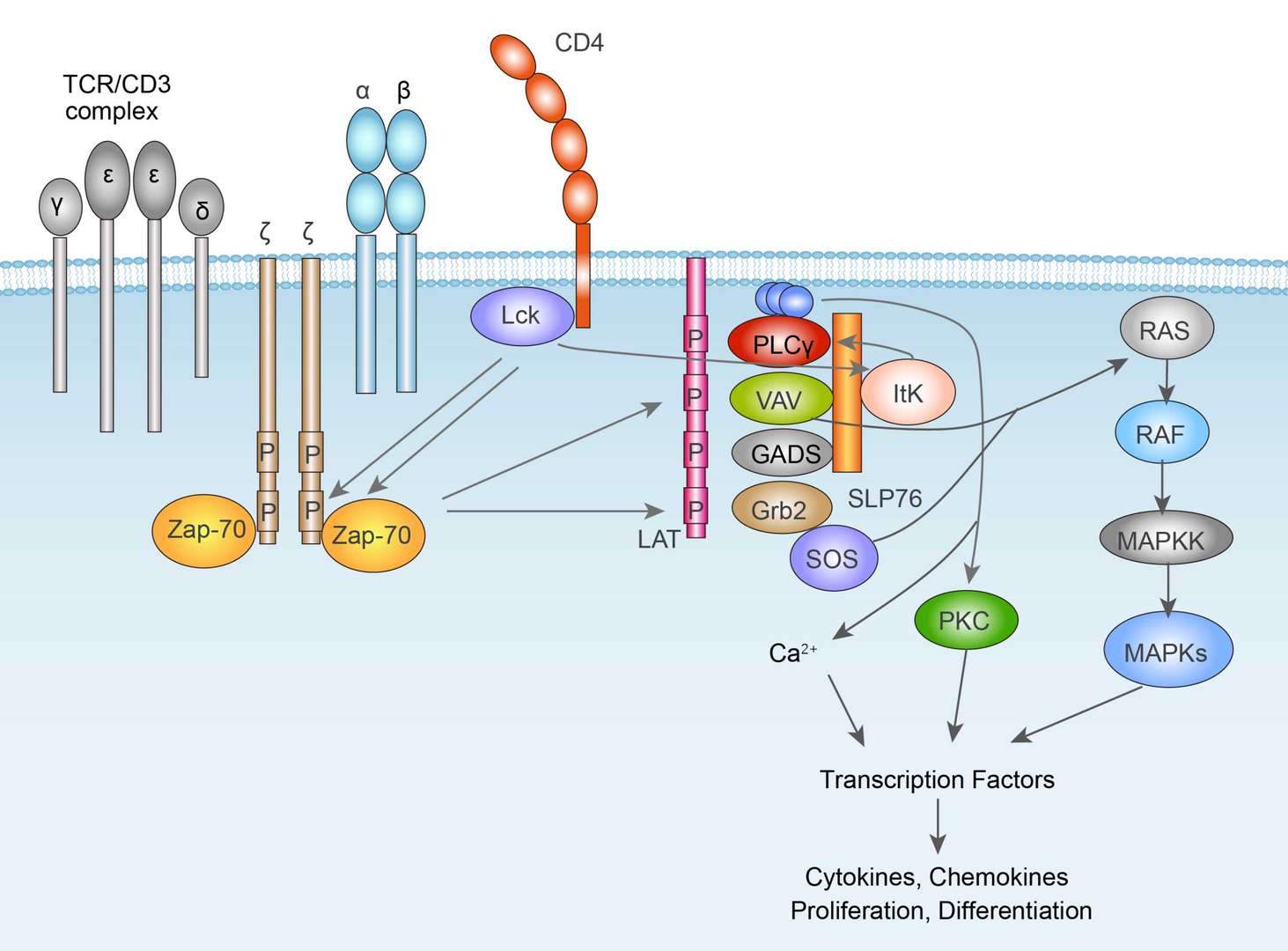 TCR Signaling Pathway
TCR Signaling Pathway
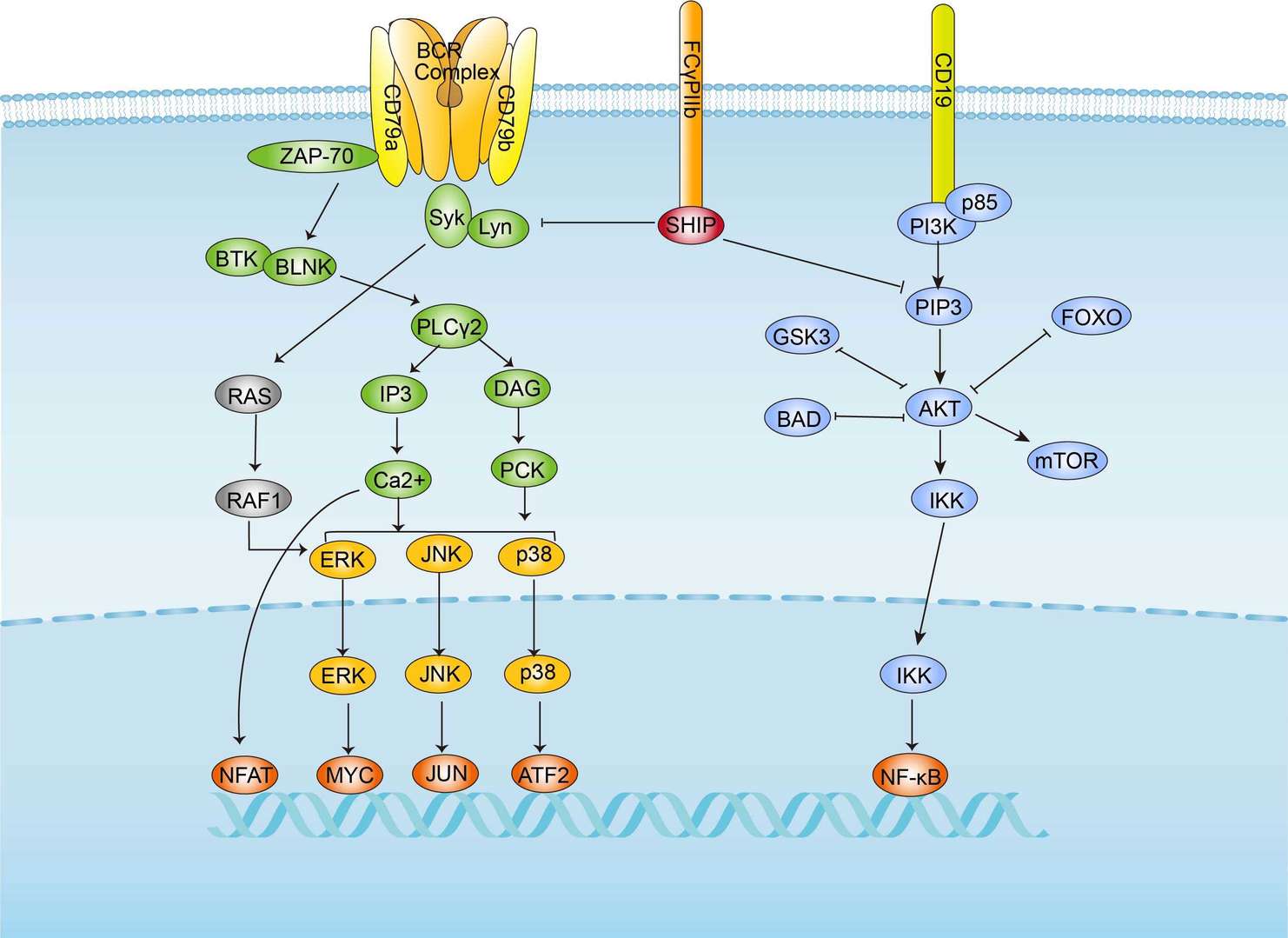 BCR Signaling Pathway
BCR Signaling PathwayCauses of GvHD
The occurrence of GvHD generally needs to meet several conditions: the graft has immune function, and there are immune cells that are normal and functional; the recipient and the donor are immunologically different in histocompatibility; the recipient is immunocompromised and cannot destroy or inactivate the transplanted cells.
After bone marrow transplantation, the T cells in the graft are introduced into the host in the form of contaminants or intentionally, and they attack the tissue of the transplant recipient after the host tissue is considered heterologous to the antigen. T cells produce excess cytokines, including TNF-α and interferon-γ (IFNγ). The widespread presence of "antigens" in the host triggers a range of immune responses, including human leukocyte antigen (HLA). Graft-versus-host disease may occur even if relatives of patients with the same HLA are used as donors, and some genetically different proteins (minor histocompatibility antigens) are presented by the major histocompatibility complex (MHC) molecules donor T cells, which treat these antigens as foreign antigens, can therefore respond immunologically.
GvHD Pathophysiology
The occurrence of GvHD is generally divided into three stages: in the afferent stage, APC (antigen presenting cells) are activated. Prior to hematopoietic stem cell transplantation, radiation or chemotherapy can cause damage and activation of host tissues, particularly the intestinal mucosa. This allows microbial products to enter and stimulate pro-inflammatory cytokines such as IL-1 and TNF-α. These pro-inflammatory cytokines increase the expression of MHC and adhesion molecules on APC, thereby increasing APC's ability to present antigens. The second phase is the efferent phase, when effector cells are activated. The activation of donor T cells further enhanced the expression of MHC and adhesion molecules, chemokines, and the expansion of CD8 + and CD4 + T cells and guest B cells. The final phase is the effector phase, where these effector cells migrate to the target organ and mediate tissue damage, leading to multiple organ failure.
GvHD Prevention and Treatment
The prevention of GvHD can start from the following aspects:
- DNA-based tissue typing can achieve more accurate HLA matching between donors and transplant patients, can reduce the incidence and severity of GvHD, and improve long-term survival.
- Umbilical cord blood (UCB) T cells are inherently immunologically immature. The use of UCB stem cells in donor transplantation that does not require T cells can reduce the incidence and severity of GvHD.
- Among the currently available drugs, cyclosporin, methotrexate and tacrolimus can prevent GvHD.
GvHD is mainly treated by intravenous injection of glucocorticoids, which can suppress T cell-mediated immune attack on host tissues. But high doses of glucocorticoids increase the risk of infection and cancer recurrence. Generally speaking, the mild GvHD symptoms appearing in the treatment of tumors can also be regarded as a craft-versus-tumor effect. When faced with the risks of GvHD, the main strategy is to focus on prevention.
For research use only. Not intended for any clinical use.
Send Inquiry
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.