

Bladder Cancer Overview
About Bladder Cancer
Bladder cancer (BCa) is the major common urethral malignancies with approximately 400,000 new cases and 165,000 deaths annually all over the world. Occurrence of bladder cancer is three to four times higher among males than among females and is the seventh most common malignancy in men and the 17th in women worldwide. Moreover, although women are less likely to develop bladder cancer, without precise reason, they generally face a worse prognosis than men. Signs and symptoms may include blood in urine (hematuria), painful urination and pelvic pain. People with bladder cancer might also experience back pain and frequent urination. There are many causes for bladder cancer, including smoking and other tobacco use, exposure to chemicals, past radiation exposure, chronic irritation of the lining of the bladder and parasitic infections. Different types of cells in your bladder can become cancerous. Urothelial carcinoma is by far the most common type of bladder cancer. Diagnosis of bladder cancer is often based on cystoscopy. This is then followed by biopsy, urine cytology or imaging tests. After confirming the bladder cancer, some additional tests are necessary to determine whether the cancer has spread to your lymph nodes or to other areas of your body, such as CT scan, magnetic resonance imaging (MRI), bone scan and chest X-ray. Screening is effective for preventing and decreasing deaths from bladder cancer. Treatments used for bladder cancer may include some combination of surgery, chemotherapy, reconstruction, radiation therapy and immunotherapy.
Overview of bladder cancer pathways
Main Signaling Pathways in Bladder Cancer
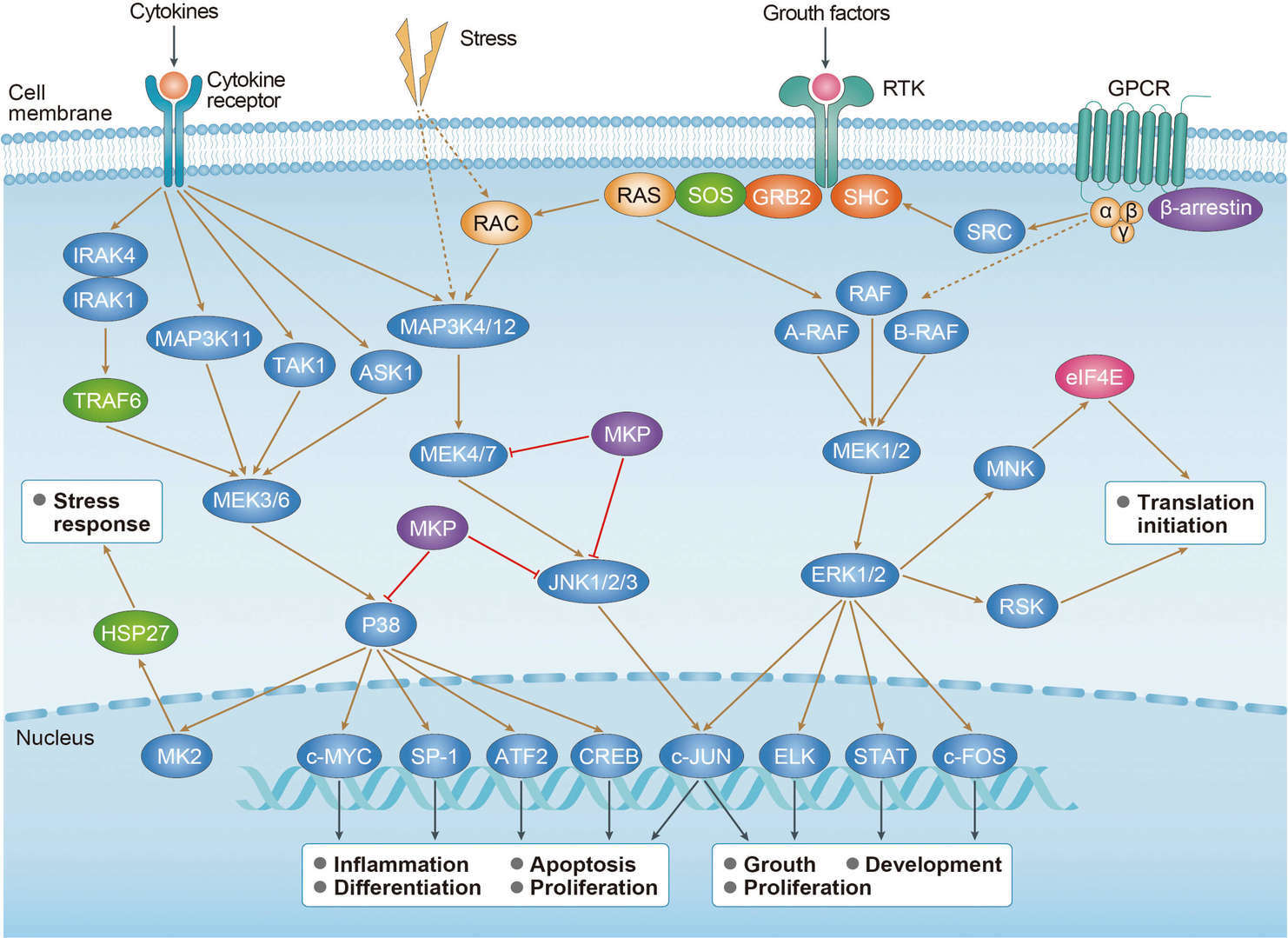 MAPK Pathway
MAPK Pathway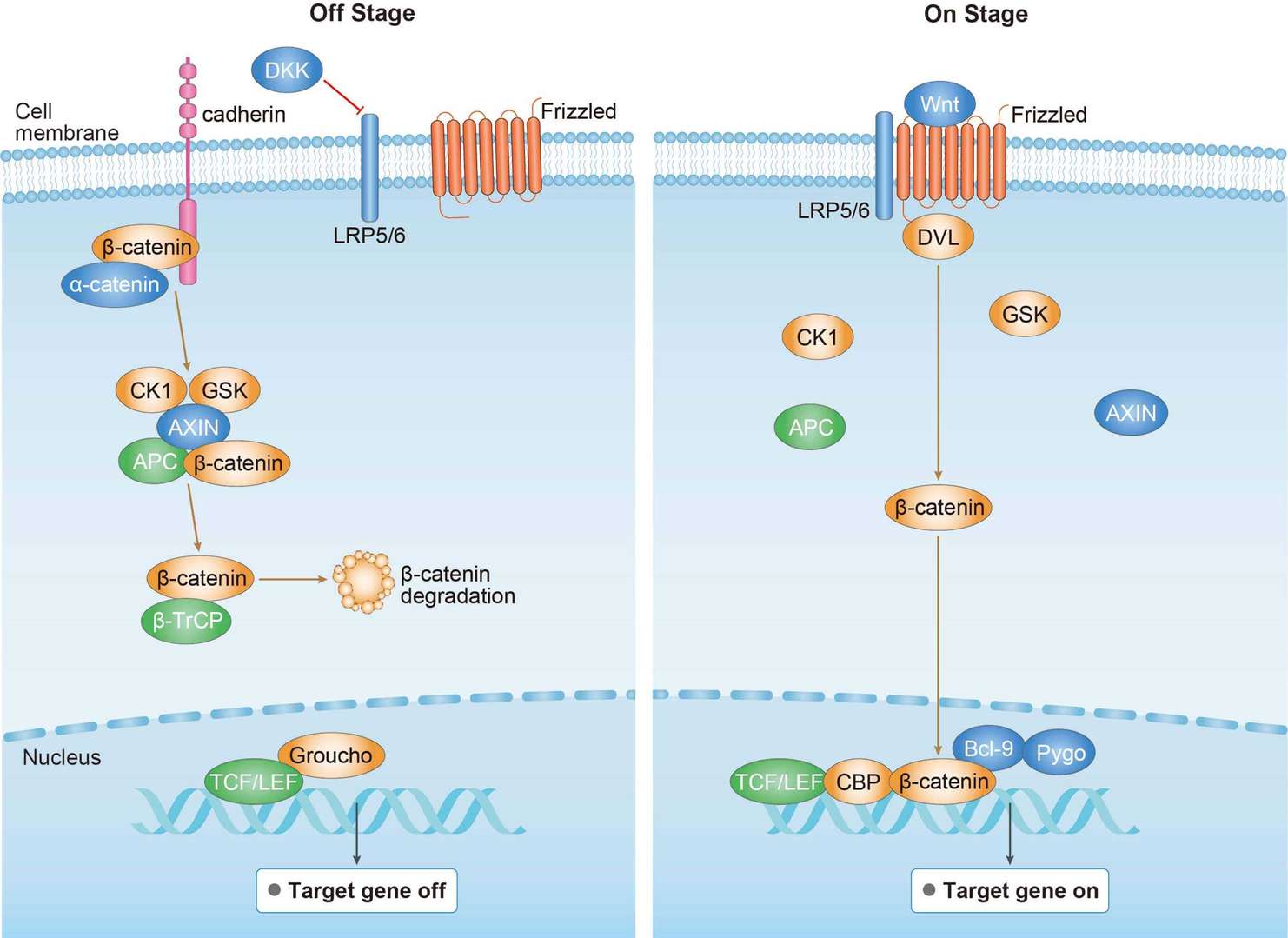 Wnt Pathway
Wnt Pathway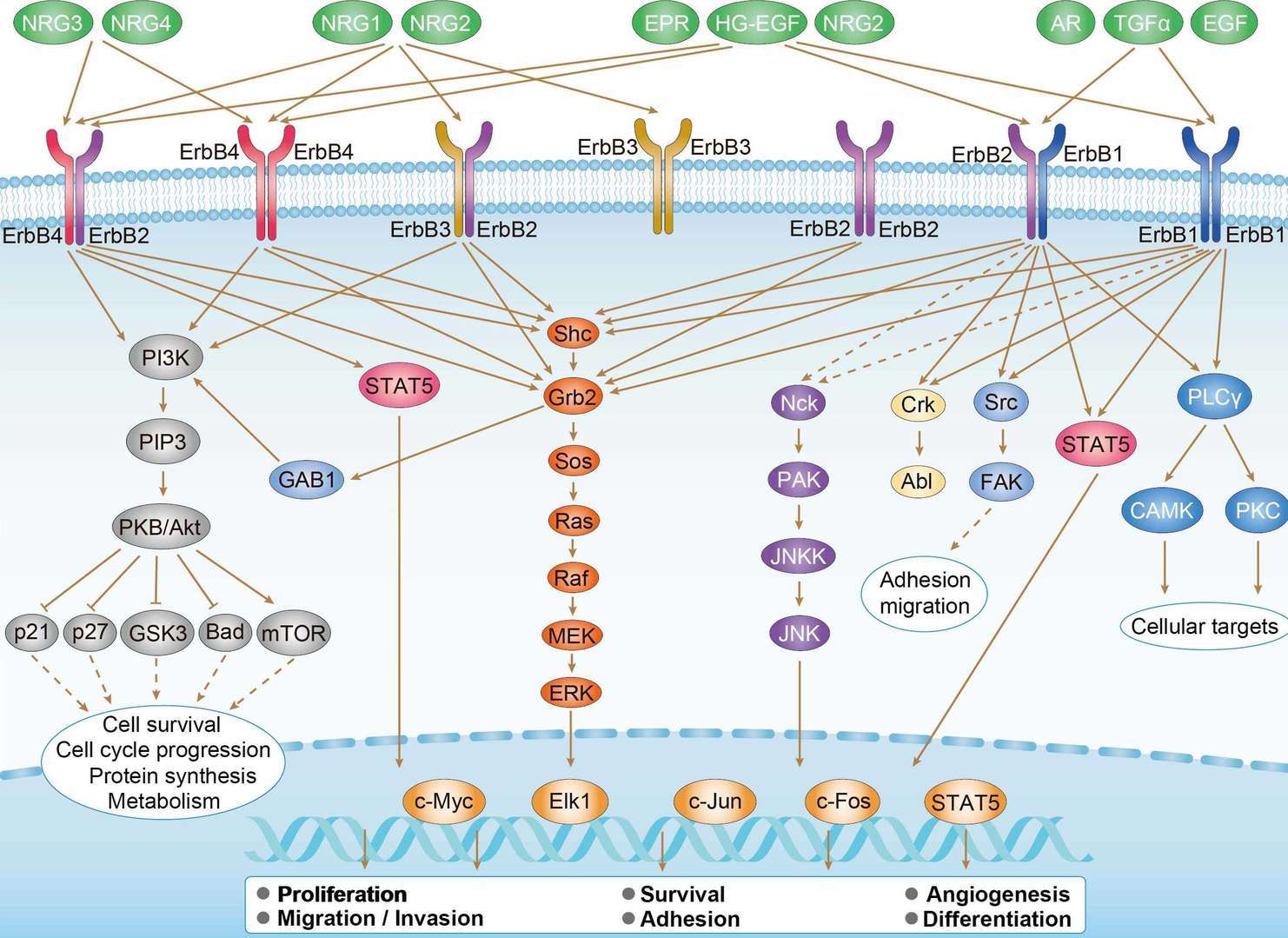 ErbB Pathway
ErbB PathwayDiagnosis of Bladder Cancer
Because bladder cancer signs and symptoms mimic those of chronic urinary tract infections, it is vital to rule this diagnosis out in any patient complaining of gross or microhematuria and/or irritative voiding symptoms. A urine specimen should be sent for both a urinalysis and urine culture to rule out an infection. In addition to the above two methods, a urine specimen should also be sent for cytology. Urine cytology evaluates for the presence of abnormal cells, which may indicate urothelial cancer. Urine cytology can aid in the initial diagnosis of bladder cancer and can also be used during routine surveillance monitoring of patients with bladder cancer. Although urine cytology is easy to obtain and highly sensitive and specific for high-grade lesions, it has a low sensitivity for low-grade lesions and a high rate of equivocal results. Because of the low sensitivity for low-grade lesions, urine cytology should be used as an adjunct test to aid in the diagnosis of bladder cancer. Another urine test used to aid in the diagnosis and surveillance of bladder cancer is the fluorescence in situ hybridization (FISH) test with urothelial cancer with a sensitivity and specificity of 72% and 83%. At the same time, FISH has the capacity to foresee recurrent disease. In addition to the above-mentioned lab tests, radiologic imaging with computed tomography (CT) scan or magnetic resonance imaging (MRI) is used to assess the kidneys, ureters, and bladder for evidence of a mass or tumor. If a bladder tumor is identified, the patient is scheduled for either a bladder biopsy or a TURBT in the OR to remove the tumor and submit it for pathologic diagnosis. When obtaining tissue samples for biopsy, it is imperative that the biopsy or TURBT specimen include detrusor muscle, as this differentiates between NMIBC and MIBC. Once the pathology results are available, the APRN can properly stage and grade the bladder cancer.
Targeted Therapy for Bladder Cancer
Targeted therapy is used to keep cancer from growing and spreading. Due to the high probability of recurrence of noninvasive BCa and poor survival rate of invasive BCa, new therapeutic approaches are needed. A cancer growth and spread are related to many growth factors pathways including the fibroblast, epidermal, and the vascular endothelial growth factor pathways. Epidermal growth factor receptor (EGFR) is a protein that helps cancer cells grow and is abundantly expressed on the surface of cancer cells. These Drugs include gefitinib, erlotinib, cetuximab and panitumumab. Human epidermal growth factor receptor 2 (HER2) initiates a variety of signaling pathways leading to cell proliferation and tumorigenesis. Drugs that target HER2 can be used to treat some bladder cancer, such as trastuzumab and lapatinib. In addition, anti-angiogenesis is also an important direction against bladder cancer. Bevacizumab, a monoclonal antibody against VEGF, has been utilized as neoadjuvant with chemotherapy. The other anti-angiogenic agents as, sunitinib, pazopanib, aflibercept and ramucirumab have been evaluated in multiple settings in urothelial carcinoma, without clear clinical benefit. Atezolizumab belongs to a class of immunotherapy drugs known as checkpoint inhibitors. It prevents a programmed cell death (PD-L1) that is found on some tumor cells from binding to another protein, PD- 1, on immune cells with subsequently immune response suppression. Cabozantinib is TKI that primarily targets MET/HGF1 which had clinical activity in patients with relapsed or refractory metastatic urothelial carcinoma with manageable toxicities.
For research use only. Not intended for any clinical use.
Send Inquiry
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.